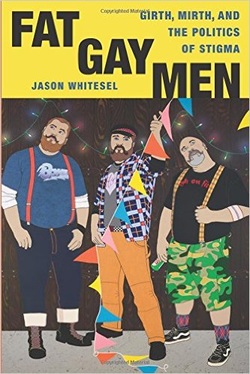
Whitsel is a partial insider (gay) as well as an outsider (thin) to this social group, and is thoughtful about his role as researcher, as well as his limited ability to critique the omnipresent fatphobia in gay culture. He is presumed (by his presence at these events) to be a "chaser," and hence explores the world of "courtesy stigma" as well as the shift in the typical power dynamics between men. Further discussions on the intersections of race and other oppressed identities are absent, and the writing does tend towards the academic; however, these narratives are a welcome change from the usual stereotypes of gay desirability and fat invisibility. Allow me to share a particularly interesting passage from his conclusion: This ethnography of Girth & Mirth culture provides a smorgasbord of strategies for dealing with the shame of fat stigma. Despite their unfortunate tendency to internalize shame and allow it to run their lives, big men continue to find more productive outlets, such as sexual objectification, status differentiation, and celebrating otherness. One of my personal favorites is campy-queer performances that utterly disregard shame, playfully acknowledging one's size in relation to one's sexuality. What a burden it is to be stigmatized, and what an admirable feat to perform one's way out of the isolation of being stigmatized. Undoubtedly, the road to acceptance appears paved with something more than simply managing stigma: it requires an unforgettable performance.
I would be delighted and grateful to hear any recommendations of other material that address this subject matter! Thank you for reading, and for anything you can share.
0 Comments
If you've been taking a closer look at your use of substances, and have decided to make some changes, you may be wondering where to start. You may not be interested in quitting, but are curious about other positive choices you could make. One of the most wonderfully liberating aspects of a harm reduction* approach is the ability to choose from an incredibly varied menu of potential change options. Here's what could be on the menu for you...  You can reduce the AMOUNT you use each time. For example:
Sometimes this is a better option for longer-acting drugs (such as heroin or alcohol), but your experience may vary. In order to go this route, you'll need to measure how much you are actually using in order to track your progress. (Additionally, please make sure you reduce slowly; if you are physically dependent on alcohol, benzodiazepines, or barbiturates, medical detox might be the safest option).  You can alter the FREQUENCY of your use, which you might do by:
This might be a good option if you find it difficult to stop using once you've started, and for substances that are shorter-acting or harder to reduce in amount (crack cocaine or speed, for example).  You can change the number or types of substances you MIX together. Much of the harm from our use comes from the way substances combine, and you can reduce negative outcomes by using just one at a time. This might initially involve paying closer attention to the reasons why you want to mix them in the first place. (You can use a decisional balance to look closer at your potential motivations and barriers.)  You can change HOW you take your substance, such as:
Routes of administration range from safer (ingesting) to less safe (smoking) to most risky (shooting), which also affects how quickly or intensely you feel the effects. You may also find that part of the complex relationship you have with a substance is an attachment to the particular ritual of using, which may require further exploration.  You can change the SITUATION that you use in. For example
This tactic is all about paying careful attention to setting, and choosing safer options.  You can put more effort into PLANNING your use, such as:
 You can try SUBSTITUTING a less harmful drug for a more harmful one:
 You can focus on OVERDOSE PREVENTION:
This may be one of the most important harm reduction techniques of all--since survival is essential for making any future positive change!  If you decide that you are going to keep using just as you are now, you can still engage in SELF-CARE while using
 Finally, if you've decided that your goal is ABSTINENCE (which qualifies as a harm reduction goal!) there is a variety of ways to get there.
There are many more safety strategies tailored to specific substances (such as only using nitrous or ketamine from a stationary position, or supplements that might be helpful following Ecstasy use). The variations are endless, and this means that you can really design a strategy that works for you! From here, you could pick out some potential options that feel feasible, and begin preparation for that particular change. This can be a complex undertaking, and you might find it helpful to have coaching or support. If you'd like more assistance, I encourage you to contact me for a consultation, and we can discuss the kinds of strategies that might work for your life. If you are just now joining me, and are curious about the harm reduction model, I invite you to check out the other posts in this series, and feel free to ask questions if you're curious. Next time, I plan to discuss some more specific tips around risk reduction and benefit maximization for psychedelic substances. Have a great week! * Some of the information in this post was gleaned from the excellent book Over the Influence: The Harm Reduction Guide for Managing Drugs and Alcohol. For those seeking further education about this topic, I can not recommend this book highly enough.  Want to make a change, but feeling stuck? Here's how to to turn awareness of both your motivations and roadblocks into a solid action plan. The DECISIONAL BALANCE is one of my favorite therapeutic tools to help folks initially explore their ambivalence about making changes. We tend to criticize ourselves for failing to take action in our lives. However, this “stuck” feeling may be a signal that we harbor some fears and doubts about the process: if you felt 100% certain that change was necessary and completely beneficial, you would have already taken action! Often our uncertainty serves as a reminder that there are important and unacknowledged factors involved; in my experience, it is usually these factors that secretly stand in our way. (This is particularly helpful in addressing substance issues, as the helpful and positive aspects of our use are often shamefully ejected from consciousness, or publicly denied.) The decisional balance is a way to honor and explore ALL your potential feelings and doubts about making change. This format goes beyond a simple pros/cons list, with power to pull out some additional information. We'll also see how there is a balance that must be tipped before any movement will occur. Here's how to begin: think about something in your life that you've been contemplating changing. You might even feel a little guilty or bad that you haven't worked on this part of your life yet.
In the first cell, please list all the benefits, pros, and positive outcomes you can think of that might result from making a change. (You can note both short-term and long-term outcomes.) In the cell below that, try to think of all the benefits, pros, and positive outcomes from NOT making a change--having things stay exactly as they are. In the top right cell, you can now list all the costs, cons, and negative outcomes that you think might occur if you made a change. Finally, in the bottom right cell, contemplate all the costs, cons, and negative outcomes you predict might happen if you do NOT change. I'll show you how this might go with someone who is considering a change in drinking behaviors:
Next, take a look back over the results. It’s important to consider not just the number of items listed in each cell, but each item’s weight, or how personally significant you rate that item. Circle or highlight the item that stands out as the most significant factor to you at this moment.
(The real key here is to focus on YOUR motivations, fears, and concerns. Your doctor would immediately target the health issues, and your partner might be concerned about the quality of your relationship, but our goal here is to get to the very heart of YOUR dilemma, and where you feel most stuck.) In the example above, if the person selected the items related to work as the most significant points (because they recently were written up for poor performance and are concerned about losing their job), our focus will be very different than if they were terrified of feeling loneliness (because they have a history of depression and self-injury, and know isolation can easily trigger an episode). Let’s now look at the item you find most compelling. Does it show us what motivates you, displaying the core value that will drive your change process? Does it point towards the barrier that we most need to address, and can we use this information as a jumping-off point to explore potential solutions or other ways to get your needs met? Brainstorm about your most significant items, and use this set of ideas to begin building your plan of action:
Before committing to change, the balance must shift towards the reasons for changing having greater weight than the reasons for maintaining the status quo. Addressing the roadblocks and narrowing in on our motivations helps us begin to tip that balance. I hope that this exercise helped you discover some new and helpful information, and I thank you for your participation! If you are just now joining me, and are curious about the Harm Reduction model, I invite you to check out the other posts in this series. Next time, I intend on laying out a potential menu of change options, which allows us to see the infinite variety of positive steps we can take towards our goals. Have a wonderful week!
Just as we have intricately complex interactions with the people and institutions around us, we all have snowflake-style unique relationships to the substances that enter our bodies. One way to examine these unique connections is through the interaction of drug, set, and setting.
Drug, obviously, is the pharmacological action of the substance itself. This can include such considerations as:
Though considerations of the substance's particular properties are necessary, they are not sufficient. There is a common tendency to reduce a drug's outcome strictly to its typical physical effects, and to see this as predictable and stable (for example, assuming alcohol will make you sociable and fun, or that cocaine inevitably leads to grandiose, manic behavior). The reality, as we shall see, is far more complex. Set (or "mindset") refers to all possible variables that YOU as a substance user bring to the table, such as:
Setting is both the physical and social environment of the use:
The dynamic interaction between these three domains can produce an infinite variety of idiosyncratic responses, and it is vital for both users and treatment providers to consider all the variables involved. From here, we can begin exploring the nuances of this interaction; a question that I commonly ask folks that I work with is: "If this was a person, what would your relationship be like?" Some possible answers might be:
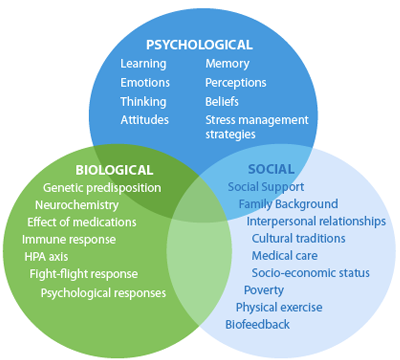
Substances can become so many things to us: lovers, friends, confidants, companions, tormentors. For those whose early lives have been lacking in attachments, they can provide a first experience of an ongoing, stable relationship. They can encourage us to freely express ourselves when we're inhibited, they can help us set boundaries with an intrusive environment, and they can give us a sense of power when we feel weak. They often offer to protect us from things we don't want to think and feel. When we tell someone struggling with substance use that they should "just QUIT, already," we miss the opportunity to explore these complexities; we have also not yet provided them with any viable alternatives to getting their needs met. Any hope for enduring change must begin with unpacking the meanings behind this most intimate of partnerships, and exploring alternative ways of caring for oneself and coping with one's life. Thanks so much for reading, and I hope this was interesting for you. Next time, I hope to delve into the heart of change/don't change ambivalence. Take care! Welcome back! In the last three parts of this series, we’ve looked at the basic principles of harm reduction, the shift away from the Moral and Disease models of addiction, and substance use as a biopsychosocial phenomenon. Today, let’s look at how this paradigm shift translates into treatment.
The assumption is that once confrontation has broken down the addictive personality, one can then be taught humility, and the personality rebuilt around sobriety. Another assumption is that addiction is the primary disease, which means that it MUST be addressed first, with total sobriety required before any other life or mental health issues are addressed. Relapse--or any deviation from total sobriety--is often grounds for discharge from the program or treatment, and the person is deemed “not ready” for treatment. Some people respond well to this structured treatment approach, and credit it with saving their lives. However, many others (especially those with severe mental health concerns or trauma histories) find this too aversive, and require alternative strategies.
In contrast, let’s look at some of the defining features of harm reduction treatment: REDEFINING SUCCESS In this model, any step in the right direction towards health, any reduction in substance-related harm, ANY POSITIVE CHANGE is seen as a success. (For example: if you generally have five drinks each night, and you then are able to bring it down to four, THAT is viewed as a step in the right direction, and recognized as a valuable accomplishment in treatment.) INDIVIDUALIZED GOAL-SETTING In contrast to the “one-size-fits-all” model of abstinence, harm reduction recommends a thorough investigation of all internal and external factors that contribute to the current situation, and the co-creation of an individualized treatment plan, based on the person's unique goals and needs. (For example: one person might have a preference for a long “warm turkey” phase of reduced use, with an eventual goal of abstinence, whereas another might just need assistance in creating a safer using plan while addressing a recent trauma.) One thing to notice here is that the wide range of possible harm reduction goals actually includes abstinence! The difference is that abstinence is not held out as the only possible goal of treatment, and it is presumed that there might be multiple and gradual ways of getting there. The emphasis here is on respecting each person’s autonomy over their life and choices, and empowering them to “run their own experiment” to determine their own optimal levels of use. FOCUS ON THE HARM, NOT THE SUBSTANCE The therapist/helper's focus is on reducing the potential harm of these substances, and not necessarily on reducing the use itself. They may provide psychoeducation about adverse medical or social consequences, along with a "menu of options" about how one might avoid those consequences. (For example, one might choose to access clean needles in order to avoid disease transmission, or to drink a glass of water for each alcoholic drink in order to avoid dehydration, or to choose a designated driver to avoid a DUI. None of these choices involve reducing one's use, but greatly enhances the safety of the situation.) SUPPORTING RELAPSE Additionally, any sort of "relapse" behavior is viewed compassionately; treatment is often re-focused here, not terminated, as this is when people are often in greatest need of support. It can serve as both a potential warning sign (were initial goals too ambitious? are there new stressors to consider?) and an opportunity for learning about one's triggers and treatment needs. Next time, we'll continue our exploration of treatment considerations with a discussion of how a person's relationship with their substance of choice affects treatment. Stay tuned, and stay well! Thanks for reading. After over a year of sharing space with some really wonderful colleagues in the ActivSpace building, I have finally moved into my own office! My new space is on the second floor, just off the building's sunny internal courtyard, and is one of the few vaulted-ceiling units in the building. I've actually been waiting specifically for one of these units to become available, as I love how the dramatic height gives a spacious feel to the room. This is difficult to capture in pictures, but I still wanted to share some images with you:
   I've taken such immense pleasure in putting together my own little cozy room, and it feels so wonderful to invite folks in to a space that feels like me.
I'm also thrilled to continue to lay down roots in the ActivSpace community, and to be part of the ever-shifting, surreal, and still vibrant Mission district, in the city I adore above all others. Thank you for reading, and for your continued support! I'm really enjoying this particular phase of my career development, and it's nice to be able to share that. Greetings again to you all! I've recently been occupied by the project of moving into my own office (news about that to follow soon), but have been wanting to return to this topic.
Before moving on to further discuss treatment, I'd like to mention an important point that's related to the biopsychosocial model: people use substances for reasons. These reasons can be viewed as pathological, or entirely normative within one’s culture and time. Here are some examples:
(This is hardly an exhaustive list--can you think of any other ones to add?) As we will see in future installments, exploring these reasons will heavily inform the direction treatment will take, and aid us in creating a compassionate frame for intervention. That's all for now! I hope to have another installment for you coming up soon. Thanks for reading! Welcome back, and thank you for your comments on my first installment in this series of posts about harm reduction! This week, we'll take a look at the larger historical context of our belief systems concerning psychoactive substances and their misuse.
The United States, in particular, has always struggled with a highly conflicted set of attitudes regarding drinking. The Puritanical roots of the colonial people, and later temperance organizations, had a hand in shaping the MORAL MODEL, seen in the 19th and early 20th centuries. This model can be characterized by these beliefs:
This was gradually (and perhaps only partially) replaced by the DISEASE MODEL, which has been viewed as our standard approach since the inception of Alcoholics Anonymous in 1935. The precepts of this model are:
In contrast, the HARM REDUCTION MODEL of substance misuse holds that:
* For example, Miller & Hester’s review of the literature on outcome studies regarding the efficacy of methods for treating alcoholism (from 1980 through 2002) concluded that, in the year following a treatment episode: - 1 in 4 remained continuously abstinent - 1 in 10 drank moderately and without problems - Mortality during this period averaged less than 2% - Even clients who DID drink in the year following treatment showed substantial improvement, abstaining on three out of four days, and reducing their overall alcohol consumption by 87% on average, with a 60% reduction in alcohol-related problems. The remarkable progress made this year towards ending our disastrous war on drugs make this an optimal time to define and discuss the concept of harm reduction*.
So what IS harm reduction, and how did it begin?
Though we can trace its roots back for several decades, harm reduction largely became visible in the 1980s as an international public health movement that recognized HIV as a larger health risk than drug use in and of itself, and aimed to reduce transmission via the distribution of condoms and clean needles. The primary principles of this health movement are an acceptance of the reality that people DO engage in high-risk behaviors, and a commitment to helping them reduce the harm associated with those behaviors, without requiring that the behaviors themselves stop. Out of these principles grow many of our well-known public safety regulations and health education programs, such as seat belt and helmet laws, minimum drinking age requirements, nicotine replacements, safer sex practices, and designated driver programs. General Philosophy Harm Reduction is a pragmatic stance, rather than one based in moral idealism, and is grounded in scientific research, human rights, compassion, and common sense. It is consumer-oriented, maintaining a low threshold for participation; providers are committed to meeting people where they ARE, rather than requiring abstinence before treatment begins. It is collaborative, rather than punitive; people are encouraged to participate in setting their own goals for treatment, and to work together with their providers towards those goals. This stance represents a major shift in how we approach individuals with high-risk behaviors, opening the doors of treatment to many more people than ever before. That's it for today--stay tuned for Part II: Moving from Away From the Moral and Disease Models! * Much of the information in these posts and my practice was gleaned not only from the excellent book Over the Influence: The Harm Reduction Guide for Managing Drugs and Alcohol, but also via live trainings with Patt Denning, Ph.D., one of the authors. For those seeking further reading in this topic, I can not recommend this book highly enough. After becoming aware of Canadian researcher Timothy A. Pychyl's blog Don't Delay, which discusses the science behind procrastination, I purchased Solving the Procrastination Puzzle: A Concise Guide to Strategies for Change, a short (by design) presentation of his team's research, formulated into practical advice on how to break our most entrenched task completion habits.
As expected, on Monday when participants were avoiding some task(s) in preference to others, we found that they typically said things like, "I'll feel more like doing that tomorrow" or "Not today. I work better under pressure." We rationalize the dissonance between our behaviors (not doing) and our expectations of ourselves (I should be doing this now). Later in the week few, if any, participants spontaneously said things like "I feel like doing that [avoided task] today" or "I'm glad I waited until tonight, because I work better like this." More surprisingly, we found a change in the participants' perceptions of their tasks. On Monday, the dreaded, avoided task was perceived as very stressful, difficult, and unpleasant. On Thursday (or make that in the wee hours of Friday morning), once they had actually engaged in the task they had avoided all week, their perceptions changed. The ratings of task stressfulness, difficulty and unpleasantness decreased significantly. What did we learn? Once we start a task, it's rarely as bad as we think. In fact, many participants made comments when we paged them during their last-minute efforts that they wished they had started earlier - the task was actually interesting, and they thought they could do a better job with a little more time. Given the large costs often involved, why, then, do we habitually procrastinate? A flash of insight occurred while reading Give in to Feel Good--another of his popular blog entries--which reframes task avoidance as an attempt at short-term mood repair. This also shed some light on the difficulty those struggling with depression and anxiety have with facing unpleasant tasks: if your mood is already low, avoidance will be a compelling short-term method to regulate your level of distress.
Like many instant gratification techniques, however, the long-term consequences eventually become greater than the immediate rewards. My clients have reported that applying the simple insight of "I don't actually have to be in the mood in order to get started on something," has been helpful in shifting their long-standing patterns of work avoidance, and thus reducing the costs of that avoidance. Check out Dr. Pychyl's blog and his book for more great insights and tips, and please feel free to share your own! * Just kidding! Therapists never procrastinate :) |
Jessica Katzman, Psy.D.I'm a psychologist with a private practice in San Francisco's Castro District. I'm interested in harm reduction, LGBTQQIAAP issues, psychedelic integration, social justice conversations, size acceptance, and any intersections of the above. I welcome your comments! 
Photo credit: Tristan Crane Photography.
Categories
All
Archives
June 2020
Disclaimer: The information and resources contained on this website are for informational purposes only and are not intended to assess, diagnose, or treat any medical and/or mental health disease or condition. The use of this website does not imply nor establish any type of therapist-client relationship. Furthermore, the information obtained from this site should not be considered a substitute for a thorough medical and/or mental health evaluation by an appropriately credentialed and licensed professional. This website includes links to other websites for informational and reference purposes only. This website does not endorse, warrant or guarantee the products, services or information described or offered at these other websites. Examine the content carefully.
|








 RSS Feed
RSS Feed