|
We’ve all struggled in our own ways to adjust to the unfolding global crisis. Though the severity of the impact varies widely, humanity is generally contending with not only the tangible disruptions in every domain of our lives, but also the loneliness and isolation in being cut off from nourishing social contact and our various communities. We may be in intense grief after losing a loved one; we may be overworked or furloughed, bored or overwhelmed, checked out or completely frazzled, anxious or depressed. We are trying our best to cope, and coping can look a lot of different ways.
1 Comment
My goal in providing this information is not to promote such use, but to assist you in doing so with the least risk and most benefit, should you choose to do so. Please see my Harm Reduction series for more information about reducing risk and habit change.
So: if your party scene involves Special K, what do you need to know to keep everyone safe as possible? (Here's one top tip: try your best not to combine it with alcohol!) Borrowing heavily from Karl Jansen’s excellent book Ketamine: Dreams and Realities (2001), let’s approach specifics for safer use of ketamine through the lens of drug, set, and setting. Here's the continuation of my psychedelics discussion. In the first part, we reviewed the resurgence of psychedelic research and how to support those having challenging experiences. As mentioned previously, you may be interested in not just preventing harm, but in getting the most out of your use of these powerful catalysts of consciousness. BENEFIT MAXIMIZATIONThe three critical elements to consider are your intention, how your intention shapes your preparation, and then integration of your experience into your everyday life.
Is your goal relational, such as enhancing intimacy and communication with your partner? If you're wanting to have a really amazing time while at an upcoming festival, your motive may be recreational. Please note that none of these intentions are better than the others (and in fact, we often have a mixture of more than one). Your planning and methods will vary, however, depending on your objective, so awareness is important. Preparation for your journey is key, and is best understood through the lens of drug, set, and setting. (See Part Five in my harm reduction series for a more extensive discussion on this topic.) DRUG: One of the best ways to trip safely is to know what you are taking. If this is a substance that is new to you, please do some research on Erowid (or other sources of quality, unbiased information) so that you are familiar with the typical effects, dosage range, and duration. It may be wise to begin on the low end of the dosage range to see how you react to this new substance. Another important factor is drug purity (for example: how much MDMA is actually in what you're taking?). Pill-testing information (for both MDMA and LSD) can be found at EcstasyData and DanceSafe. Interactions are also extremely important; Zendo volunteers have shared that many of the folks who end up there for assistance have mixed multiple (often unknown) substances together. Again, if you are on any medications, please check in with a health care professional (and do your research) before using psychoactive drugs! SET: Psychedelics are thought of as "non-specific amplifiers," meaning that they can greatly enhance the perception of whatever is already happening for you. Consider your current state: did you just have a difficult breakup and haven't slept for three days? Worried about losing your job? That content will likely come up, so be ready for it. (This may be intentional for those using the medicine therapeutically, but can cause discomfort for those looking to use recreationally.) Awareness of your own personal and family history of mental health is also very important, as those with psychotic or bipolar vulnerabilities may have adverse reactions to these substances. SETTING: Psychedelics are unique in how they sensitize us so exquisitely to our environment, which means that our surroundings crucially shape our journey. Knowing that we will be in a highly suggestible state can help us decide where we want to be and who to have around. Many choose to create rituals to begin and close their journeys, and surround themselves with stimulating artwork or meaningful objects. They plan special music playlists to help guide them through the experience. They trip outdoors in nature, or in private, safe accommodations without risk of interruption. It is also helpful to be deliberate about who else will be involved in your experience. You may choose to be with a intimate partner, or a group of close friends; it can be helpful to make an agreement with everyone beforehand on how to handle difficult experiences. (If there isn't enough trust built to have such a conversation, you might think twice about tripping with these folks!) There are longstanding traditions involving the use of a shaman, trip sitter, guide, therapist, coach, ground control, or otherwise sober person during these journeys. Many feel that they are able to let go and travel to much deeper places when a guide provides a stabilizing, grounding force. Plant medicine use in indigenous cultures tends to be highly ritualized and directed by an elder or shaman, which can help contain the powerful material that can arise. If you are curious about using a sitter, I highly recommend James Fadiman's excellent book The Psychedelic Explorer's Guide, which describes in detail the best practices for guiding/being guided on safe, sacred entheogenic journeys. (Another great collection of resources about trip-sitting can be found here, and you can read the relevant chapters of Fadiman's book in this pdf.) PUTTING IT ALL TOGETHER: let's say your intention is to enhance your enjoyment of a concert with friends. Great! In that case, you might choose a lower dose (i.e. a "museum dose") in order to best facilitate dancing and crowd navigation. You could check in with your friends to see if they will be similarly tripping (or to designate a sober trip-wrangler), and to make a safety plan for the evening. You might also want to be sure that your mental health feels optimal, with no acute stressors, as well as being well-rested and adequately fed before you begin. Make sure you have regular access to water at your event, and pay attention to temperature regulation. Don't operate a motor vehicle. Have fun! However, if your intention is to address longstanding PTSD symptoms and facilitate the healing process, you may choose a much higher dose, and plan both preparatory and follow-up therapy sessions to lay the groundwork for the journey.
Finally, let's now turn to the importance of integration. These medicines can bring profound improvement to our lives when we bring the insights gained during the trip back into our everyday world. A period of introspection following the journey is highly recommended, especially for those with therapeutic and spiritual aims, so giving adequate time for this unfolding is important. There are multiple ways to reflect on your session: journaling about your experience (especially while reviewing your initial intentions), speaking with someone you trust and who understands psychedelic use, creative expression, attending a local integration group, bodywork, meditation, yoga, or spending time in nature. A growing number of therapists are now beginning to offer integration services, and I am happy to be one of them! You may contact me to find out more about how I work, and if I might be a good candidate for your support team. That's all for now! I hope you enjoyed my tiny sample of this immense topic, and please let me know if you have any questions or want to discuss this matter more. Thanks for reading. Disclaimer: These substances remain illegal in many jurisdictions, and this site does not recommend the activities described here. This information is provided for educational purposes only, and to assist those who have already decided to use substances to do it in the safest and most beneficial manner possible. It is your responsibility to assume the risks associated with these activities. Please consult with a medical professional beforehand, especially if you have a preexisting physical or mental/emotional concerns, or are on medication. Psychedelic-assisted therapy is legal only in approved research settings, and I am unable to offer such services at this time.
Welcome back! The next two installments in my harm reduction series concern strategies and techniques best used with psychedelics (such as LSD and mushrooms) and empathogens (such as MDMA). The mainstream media (such as this illuminating New Yorker article by Michael Pollan) has recently given much attention to the resurgence of research on psychedelic- and empathogen-assisted psychotherapy, and the promising results being obtained in treating PTSD, depression, end-of-life anxiety, substance misuse, and other forms of distress. Additionally, a new generation of enthusiasts are buzzing about the magic of microdosing. Many of us in the field are eagerly awaiting our renewed ability (following decades of restrictions) to make use of these powerful change agents, and in the meantime, are attending international conferences and certificate training programs in anticipation of a post-prohibition world.
HARM REDUCTION In response to the needs of our community, organizations such as the Zendo Project aim to create safe, calm environments with trained volunteers to support psychedelic users having difficult experiences, preventing the automatic intervention of law enforcement or medical services.
The Zendo Project has successfully staffed numerous festivals--such as Burning Man and Lightning in a Bottle--since 2012. I've been inspired by their work, and would like to share some of the most important points here. If you happen to encounter someone who is having a difficult trip and are able to assist them, begin by asking about any physical complaints which might necessitate medical attention. You may then find out what they've taken, how much, when they took it, and if they are on any other medications or substances (including alcohol) that might interact. You might then support them using these four principles: 1) Safe Space: These substances often enhance perception, making us extraordinarily sensitive to our environment, and we can easily become overwhelmed by sensory and interpersonal input. If someone is having a challenging experience, you may attempt to move them to a setting that is quiet and comfortable, with enough space for them to feel at ease. Adjust temperatures if they are too hot or cold, and offer water. Soft music and dim lights are helpful. 2) Sitting, Not Guiding: Provide a calm, reassuring, non-directive presence, without feeling the need to "fix" anything. Respond when needed, but don't take over; allow their unfolding experience to guide. Just be with, listen, and observe. Encourage any expression that needs to happen (via conversation, art, dance, movement, sound, etc). 3) Talk Through, Not Down: Help them connect with their feelings, and invite them to gently explore, rather than resist; most difficult experiences are a result of fighting what's happening during the trip. If it is helpful, you may remind them, when needed, that (a) they have taken a drug, and its effects will pass before too long and (b) they are safe where they are, and any medical needs will be attended to. 4) Difficult Is Not the Same As Bad: Where appropriate, you may remind them that many other people have had similar trips, and that challenging experiences often lead to learning and growth. Encourage them to face their experience with curiosity about why these feelings are arising now. (Do you want to see a role-play video of these techniques? Sure, why not?) The intervention of medical or security staff still remains an option in extreme cases, but many are able to resolve their difficult experiences fairly organically and positively when given this type of support. These principles can help someone who is in the middle of a challenging trip, and you might recall them for yourself as needed. (Full credit and gratitude to the Multidisciplinary Association for Psychedelic Studies and to Zendo, a MAPS project, for this important information!) However, perhaps you want both tools to troubleshoot problems, and tips on how to have the most positive experience possible. Benefit maximization is just as important as harm reduction, and I'll cover that in my next post. Go here for the next bite-sized bit on this topic!
If you've been taking a closer look at your use of substances, and have decided to make some changes, you may be wondering where to start. You may not be interested in quitting, but are curious about other positive choices you could make. One of the most wonderfully liberating aspects of a harm reduction* approach is the ability to choose from an incredibly varied menu of potential change options. Here's what could be on the menu for you...  You can reduce the AMOUNT you use each time. For example:
Sometimes this is a better option for longer-acting drugs (such as heroin or alcohol), but your experience may vary. In order to go this route, you'll need to measure how much you are actually using in order to track your progress. (Additionally, please make sure you reduce slowly; if you are physically dependent on alcohol, benzodiazepines, or barbiturates, medical detox might be the safest option).  You can alter the FREQUENCY of your use, which you might do by:
This might be a good option if you find it difficult to stop using once you've started, and for substances that are shorter-acting or harder to reduce in amount (crack cocaine or speed, for example).  You can change the number or types of substances you MIX together. Much of the harm from our use comes from the way substances combine, and you can reduce negative outcomes by using just one at a time. This might initially involve paying closer attention to the reasons why you want to mix them in the first place. (You can use a decisional balance to look closer at your potential motivations and barriers.)  You can change HOW you take your substance, such as:
Routes of administration range from safer (ingesting) to less safe (smoking) to most risky (shooting), which also affects how quickly or intensely you feel the effects. You may also find that part of the complex relationship you have with a substance is an attachment to the particular ritual of using, which may require further exploration.  You can change the SITUATION that you use in. For example
This tactic is all about paying careful attention to setting, and choosing safer options.  You can put more effort into PLANNING your use, such as:
 You can try SUBSTITUTING a less harmful drug for a more harmful one:
 You can focus on OVERDOSE PREVENTION:
This may be one of the most important harm reduction techniques of all--since survival is essential for making any future positive change!  If you decide that you are going to keep using just as you are now, you can still engage in SELF-CARE while using
 Finally, if you've decided that your goal is ABSTINENCE (which qualifies as a harm reduction goal!) there is a variety of ways to get there.
There are many more safety strategies tailored to specific substances (such as only using nitrous or ketamine from a stationary position, or supplements that might be helpful following Ecstasy use). The variations are endless, and this means that you can really design a strategy that works for you! From here, you could pick out some potential options that feel feasible, and begin preparation for that particular change. This can be a complex undertaking, and you might find it helpful to have coaching or support. If you'd like more assistance, I encourage you to contact me for a consultation, and we can discuss the kinds of strategies that might work for your life. If you are just now joining me, and are curious about the harm reduction model, I invite you to check out the other posts in this series, and feel free to ask questions if you're curious. Next time, I plan to discuss some more specific tips around risk reduction and benefit maximization for psychedelic substances. Have a great week! * Some of the information in this post was gleaned from the excellent book Over the Influence: The Harm Reduction Guide for Managing Drugs and Alcohol. For those seeking further education about this topic, I can not recommend this book highly enough.  Want to make a change, but feeling stuck? Here's how to to turn awareness of both your motivations and roadblocks into a solid action plan. The DECISIONAL BALANCE is one of my favorite therapeutic tools to help folks initially explore their ambivalence about making changes. We tend to criticize ourselves for failing to take action in our lives. However, this “stuck” feeling may be a signal that we harbor some fears and doubts about the process: if you felt 100% certain that change was necessary and completely beneficial, you would have already taken action! Often our uncertainty serves as a reminder that there are important and unacknowledged factors involved; in my experience, it is usually these factors that secretly stand in our way. (This is particularly helpful in addressing substance issues, as the helpful and positive aspects of our use are often shamefully ejected from consciousness, or publicly denied.) The decisional balance is a way to honor and explore ALL your potential feelings and doubts about making change. This format goes beyond a simple pros/cons list, with power to pull out some additional information. We'll also see how there is a balance that must be tipped before any movement will occur. Here's how to begin: think about something in your life that you've been contemplating changing. You might even feel a little guilty or bad that you haven't worked on this part of your life yet.
In the first cell, please list all the benefits, pros, and positive outcomes you can think of that might result from making a change. (You can note both short-term and long-term outcomes.) In the cell below that, try to think of all the benefits, pros, and positive outcomes from NOT making a change--having things stay exactly as they are. In the top right cell, you can now list all the costs, cons, and negative outcomes that you think might occur if you made a change. Finally, in the bottom right cell, contemplate all the costs, cons, and negative outcomes you predict might happen if you do NOT change. I'll show you how this might go with someone who is considering a change in drinking behaviors:
Next, take a look back over the results. It’s important to consider not just the number of items listed in each cell, but each item’s weight, or how personally significant you rate that item. Circle or highlight the item that stands out as the most significant factor to you at this moment.
(The real key here is to focus on YOUR motivations, fears, and concerns. Your doctor would immediately target the health issues, and your partner might be concerned about the quality of your relationship, but our goal here is to get to the very heart of YOUR dilemma, and where you feel most stuck.) In the example above, if the person selected the items related to work as the most significant points (because they recently were written up for poor performance and are concerned about losing their job), our focus will be very different than if they were terrified of feeling loneliness (because they have a history of depression and self-injury, and know isolation can easily trigger an episode). Let’s now look at the item you find most compelling. Does it show us what motivates you, displaying the core value that will drive your change process? Does it point towards the barrier that we most need to address, and can we use this information as a jumping-off point to explore potential solutions or other ways to get your needs met? Brainstorm about your most significant items, and use this set of ideas to begin building your plan of action:
Before committing to change, the balance must shift towards the reasons for changing having greater weight than the reasons for maintaining the status quo. Addressing the roadblocks and narrowing in on our motivations helps us begin to tip that balance. I hope that this exercise helped you discover some new and helpful information, and I thank you for your participation! If you are just now joining me, and are curious about the Harm Reduction model, I invite you to check out the other posts in this series. Next time, I intend on laying out a potential menu of change options, which allows us to see the infinite variety of positive steps we can take towards our goals. Have a wonderful week!
Just as we have intricately complex interactions with the people and institutions around us, we all have snowflake-style unique relationships to the substances that enter our bodies. One way to examine these unique connections is through the interaction of drug, set, and setting.
Drug, obviously, is the pharmacological action of the substance itself. This can include such considerations as:
Though considerations of the substance's particular properties are necessary, they are not sufficient. There is a common tendency to reduce a drug's outcome strictly to its typical physical effects, and to see this as predictable and stable (for example, assuming alcohol will make you sociable and fun, or that cocaine inevitably leads to grandiose, manic behavior). The reality, as we shall see, is far more complex. Set (or "mindset") refers to all possible variables that YOU as a substance user bring to the table, such as:
Setting is both the physical and social environment of the use:
The dynamic interaction between these three domains can produce an infinite variety of idiosyncratic responses, and it is vital for both users and treatment providers to consider all the variables involved. From here, we can begin exploring the nuances of this interaction; a question that I commonly ask folks that I work with is: "If this was a person, what would your relationship be like?" Some possible answers might be:
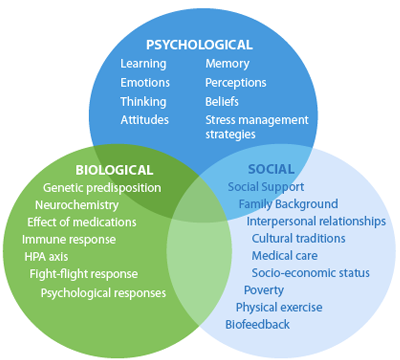
Substances can become so many things to us: lovers, friends, confidants, companions, tormentors. For those whose early lives have been lacking in attachments, they can provide a first experience of an ongoing, stable relationship. They can encourage us to freely express ourselves when we're inhibited, they can help us set boundaries with an intrusive environment, and they can give us a sense of power when we feel weak. They often offer to protect us from things we don't want to think and feel. When we tell someone struggling with substance use that they should "just QUIT, already," we miss the opportunity to explore these complexities; we have also not yet provided them with any viable alternatives to getting their needs met. Any hope for enduring change must begin with unpacking the meanings behind this most intimate of partnerships, and exploring alternative ways of caring for oneself and coping with one's life. Thanks so much for reading, and I hope this was interesting for you. Next time, I hope to delve into the heart of change/don't change ambivalence. Take care! Welcome back! In the last three parts of this series, we’ve looked at the basic principles of harm reduction, the shift away from the Moral and Disease models of addiction, and substance use as a biopsychosocial phenomenon. Today, let’s look at how this paradigm shift translates into treatment.
The assumption is that once confrontation has broken down the addictive personality, one can then be taught humility, and the personality rebuilt around sobriety. Another assumption is that addiction is the primary disease, which means that it MUST be addressed first, with total sobriety required before any other life or mental health issues are addressed. Relapse--or any deviation from total sobriety--is often grounds for discharge from the program or treatment, and the person is deemed “not ready” for treatment. Some people respond well to this structured treatment approach, and credit it with saving their lives. However, many others (especially those with severe mental health concerns or trauma histories) find this too aversive, and require alternative strategies.
In contrast, let’s look at some of the defining features of harm reduction treatment: REDEFINING SUCCESS In this model, any step in the right direction towards health, any reduction in substance-related harm, ANY POSITIVE CHANGE is seen as a success. (For example: if you generally have five drinks each night, and you then are able to bring it down to four, THAT is viewed as a step in the right direction, and recognized as a valuable accomplishment in treatment.) INDIVIDUALIZED GOAL-SETTING In contrast to the “one-size-fits-all” model of abstinence, harm reduction recommends a thorough investigation of all internal and external factors that contribute to the current situation, and the co-creation of an individualized treatment plan, based on the person's unique goals and needs. (For example: one person might have a preference for a long “warm turkey” phase of reduced use, with an eventual goal of abstinence, whereas another might just need assistance in creating a safer using plan while addressing a recent trauma.) One thing to notice here is that the wide range of possible harm reduction goals actually includes abstinence! The difference is that abstinence is not held out as the only possible goal of treatment, and it is presumed that there might be multiple and gradual ways of getting there. The emphasis here is on respecting each person’s autonomy over their life and choices, and empowering them to “run their own experiment” to determine their own optimal levels of use. FOCUS ON THE HARM, NOT THE SUBSTANCE The therapist/helper's focus is on reducing the potential harm of these substances, and not necessarily on reducing the use itself. They may provide psychoeducation about adverse medical or social consequences, along with a "menu of options" about how one might avoid those consequences. (For example, one might choose to access clean needles in order to avoid disease transmission, or to drink a glass of water for each alcoholic drink in order to avoid dehydration, or to choose a designated driver to avoid a DUI. None of these choices involve reducing one's use, but greatly enhances the safety of the situation.) SUPPORTING RELAPSE Additionally, any sort of "relapse" behavior is viewed compassionately; treatment is often re-focused here, not terminated, as this is when people are often in greatest need of support. It can serve as both a potential warning sign (were initial goals too ambitious? are there new stressors to consider?) and an opportunity for learning about one's triggers and treatment needs. Next time, we'll continue our exploration of treatment considerations with a discussion of how a person's relationship with their substance of choice affects treatment. Stay tuned, and stay well! Thanks for reading. Greetings again to you all! I've recently been occupied by the project of moving into my own office (news about that to follow soon), but have been wanting to return to this topic.
Before moving on to further discuss treatment, I'd like to mention an important point that's related to the biopsychosocial model: people use substances for reasons. These reasons can be viewed as pathological, or entirely normative within one’s culture and time. Here are some examples:
(This is hardly an exhaustive list--can you think of any other ones to add?) As we will see in future installments, exploring these reasons will heavily inform the direction treatment will take, and aid us in creating a compassionate frame for intervention. That's all for now! I hope to have another installment for you coming up soon. Thanks for reading! Welcome back, and thank you for your comments on my first installment in this series of posts about harm reduction! This week, we'll take a look at the larger historical context of our belief systems concerning psychoactive substances and their misuse.
The United States, in particular, has always struggled with a highly conflicted set of attitudes regarding drinking. The Puritanical roots of the colonial people, and later temperance organizations, had a hand in shaping the MORAL MODEL, seen in the 19th and early 20th centuries. This model can be characterized by these beliefs:
This was gradually (and perhaps only partially) replaced by the DISEASE MODEL, which has been viewed as our standard approach since the inception of Alcoholics Anonymous in 1935. The precepts of this model are:
In contrast, the HARM REDUCTION MODEL of substance misuse holds that:
* For example, Miller & Hester’s review of the literature on outcome studies regarding the efficacy of methods for treating alcoholism (from 1980 through 2002) concluded that, in the year following a treatment episode: - 1 in 4 remained continuously abstinent - 1 in 10 drank moderately and without problems - Mortality during this period averaged less than 2% - Even clients who DID drink in the year following treatment showed substantial improvement, abstaining on three out of four days, and reducing their overall alcohol consumption by 87% on average, with a 60% reduction in alcohol-related problems. |
Jessica Katzman, Psy.D.I'm a psychologist with a private practice in San Francisco's Castro District. I'm interested in harm reduction, LGBTQQIAAP issues, psychedelic integration, social justice conversations, size acceptance, and any intersections of the above. I welcome your comments! 
Photo credit: Tristan Crane Photography.
Categories
All
Archives
June 2020
Disclaimer: The information and resources contained on this website are for informational purposes only and are not intended to assess, diagnose, or treat any medical and/or mental health disease or condition. The use of this website does not imply nor establish any type of therapist-client relationship. Furthermore, the information obtained from this site should not be considered a substitute for a thorough medical and/or mental health evaluation by an appropriately credentialed and licensed professional. This website includes links to other websites for informational and reference purposes only. This website does not endorse, warrant or guarantee the products, services or information described or offered at these other websites. Examine the content carefully.
|








 RSS Feed
RSS Feed