|
This week seemed to evoke less of those massive-tectonic-plate-shifts in the collective, and hence had more of a Minor Arcana feel for me. A friend wisely described this moment as “the calm between two storms,” which inspired this offering: SIX OF SWORDS 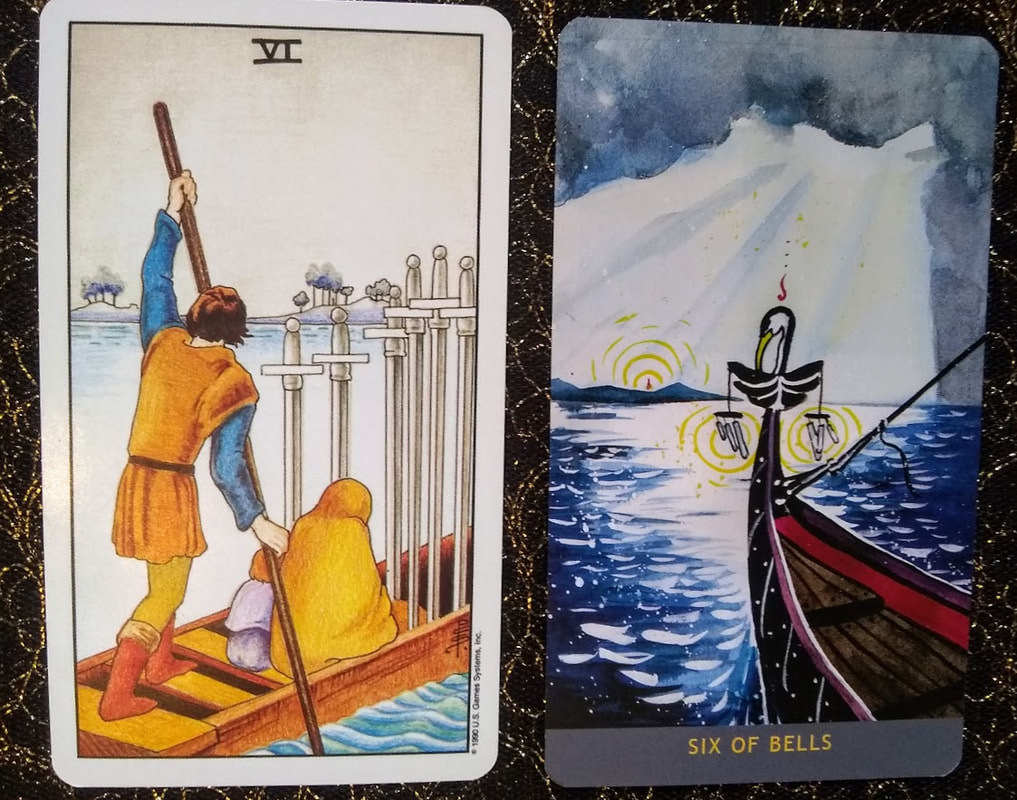 This card depicts moments where we are coping with or recovering from a painful ordeal, while still carrying the burden of difficult memories or past baggage. We feel numb, disengaged, and listless; we may be functional, but not exactly thriving. The image here is of somber passage through a troubled time; a transition between two shores. We are not entirely out of the choppy, rough currents yet, but may be able to see calmer waters ahead. There is some hope that the difficult choices we’ve had to make, and the hardships we’ve endured, will eventually lead to a better path, even if there are no overnight solutions or immediate transformations available. In any case, we are leaving behind what is familiar, and so we may notice a sense of loss, even as we begin to pick up the pieces. Whenever multiple figures appear on a card, we are prompted to think about which ones we identify with most. Are we the huddled, mourning passengers, unable to see through the dense thicket of troubled thoughts obscuring our view? Are we steering the boat, using our elevated perspective to assist others through this rite of passage? Or is this--as parts-oriented therapists like myself so love as an interpretation--a portrayal of an inner state, wherein we are both the helper and the one needing support? Perhaps there is a part of us that is contracted with sadness, unable to step back from the ruminative cycles of worry, regret, and anguish; there may also be a part of us that has some clarity, and can help steer our ship through the agitated waves. This image has a quiet heaviness to it, and yet also invites us to begin getting some distance from a troubled past; to think about what to keep and what to leave behind. It also hints that we may want to reach out for help as we sort through this, whether that means venting to a friend, entering therapy, or simply calling upon the sturdier, wiser parts of ourselves for guidance. (Cards pictured here are from the Universal Waite, a recolored version of the Rider-Waite-Smith deck, and the Numinous Tarot, a radical deck with diverse representations and gender-neutral language.)
0 Comments
Hello, friends. Another week, another archetypal shift in our collective reality... The random thought “Corona virus may well be a master class in Being With What Is,” percolated up few days ago, and so this particular archetype made its presence known: THE HANGED ONE  This card can represent situations in which we voluntarily tolerate discomfort, consciously sacrificing our self-interest to prioritize a greater purpose. We delay gratification, suspend action, and ready ourselves for a period of transition ahead. However, this image also suggests a possible stance that may help us hang in there with difficult moments. We have an opportunity here to drop the struggle, surrender to what is, accept our current reality, and practice patient serenity. (Note: accept does not mean like or endorse. It simply means validating reality as it is, and releasing our insistence that things be otherwise.) The other opportunity this archetype provides is via its iconic reversal, as we allow this inversion to provide new perspectives. When our world gets turned upside down, we suddenly see things from a new angle, and here again (much like in the Tower) we have an opportunity to question old belief systems and disrupt our habits. Shadow elements of this pattern may manifest in martyrdom, passivity, and a sense of being stuck, apathetic, or asleep to existence. Conversely, we may also notice moments of resistance and intense struggle around our lack of control. (From a somatic/trauma-informed lens, it makes total and complete sense that our nervous systems may activate around feeling being trapped against our will by engaging in a FIGHT response, or by shifting into collapsed numbness.) For counsel, I turn to brilliant, queer, witchy writer and San Francisco icon Michelle Tea, who writes: If Hanged Man has come up for you, know that everything is in motion, even if it feels like nothing is moving. That’s the nature of the Hanged Man. It’s a waiting game, and the waiting can be interminable. It’s not a time for activity. If you’re considering making a move to help a situation along, don’t. You’ll probably just mess it up. If you’ve been insulted or threatened, the best recourse under the Hanged Man is to lay low and wait it out. Passivity is rewarded. Don’t send that email, don’t hit back. Just scramble up that tree, get yourself in the most comfortable position you can, and count your breaths until the situation remedies itself. And it will. Movement is always occurring within the Hanged Man; it’s just happening away from you, or so deep inside of you that you can’t see it clearly. So in order to move through this phase, we settle the best we can into our self-imposed purgatory, relax into our discomfort, and try to take in the new outlook we now have on existence. Additionally, if you are noticing more intense edges around bodily activation, or if you are processing a trauma response, you may experiment with somatic mindfulness exercises to begin regulating your nervous system. Please do reach out and contact a professional if you need more assistance with this, and take good care of yourself! (Cards pictured here are from the Universal Waite, a recolored version of the Rider-Waite-Smith deck, and the Numinous Tarot, a radical deck with diverse representations and gender-neutral language.)
Sharing another card whose energies I also felt moving through the world last week, twinned with the Tower, and which I see still spilling over into this one. THE HERMIT  This card iconically captures moments of quiet solitude and seclusion, where we withdraw from everyday life and material concerns, initiating periods of deep introspection, contemplation, and inner-focused exploration. When these forces emerge, we are called to ask bigger, broader existential questions about the purpose and meaning of our lives. We go on vision quests or attend artistic or silent retreats. We meditate, enter psychoanalysis, or engage in dreamwork, giving voice to the hidden parts of the psyche that can only be heard in conditions of quiet stillness. This card’s imagery also evokes an archetypal wisdom figure who helps guide others through their inner process. This is the teacher, sage, guru, mentor, therapist, or sponsor who offers us direction, having walked their own difficult path, and now holding a beacon out for us to follow. This may be an external process, in which we seek out a teacher, or step into our own role in guiding others. This may also be a completely internal dynamic, as you are invited to make contact with your own inner guides. Psychedelic assisted therapy frequently refers to “inner healing intelligence,” and practitioners are trained to set aside their agendas and allow this force to do the work. Like all powerful archetypes, we may notice where it begins to tip over into its shadow. Under the influence of the Hermit, we can be swept away by fears about the outside world or social paranoia, and move into extreme isolation and avoidance. We may shut down into ruminative depression, refusing to participate in life. In moments of discernment, we can ask ourselves: am I looking inward in an attempt to find or discover something, or turning away to escape something? (Cards pictured here are from the Universal Waite, a recolored version of the Rider-Waite-Smith deck, and the Numinous Tarot, a radical deck with diverse representations and gender-neutral language.)
We seem to be moving through a season that brings deeper existential narratives to the surface, and so my mind turns to the expansive archetypes so artfully symbolized by the Major Arcana of the tarot. I will share here with you the card this week inspired: THE TOWER 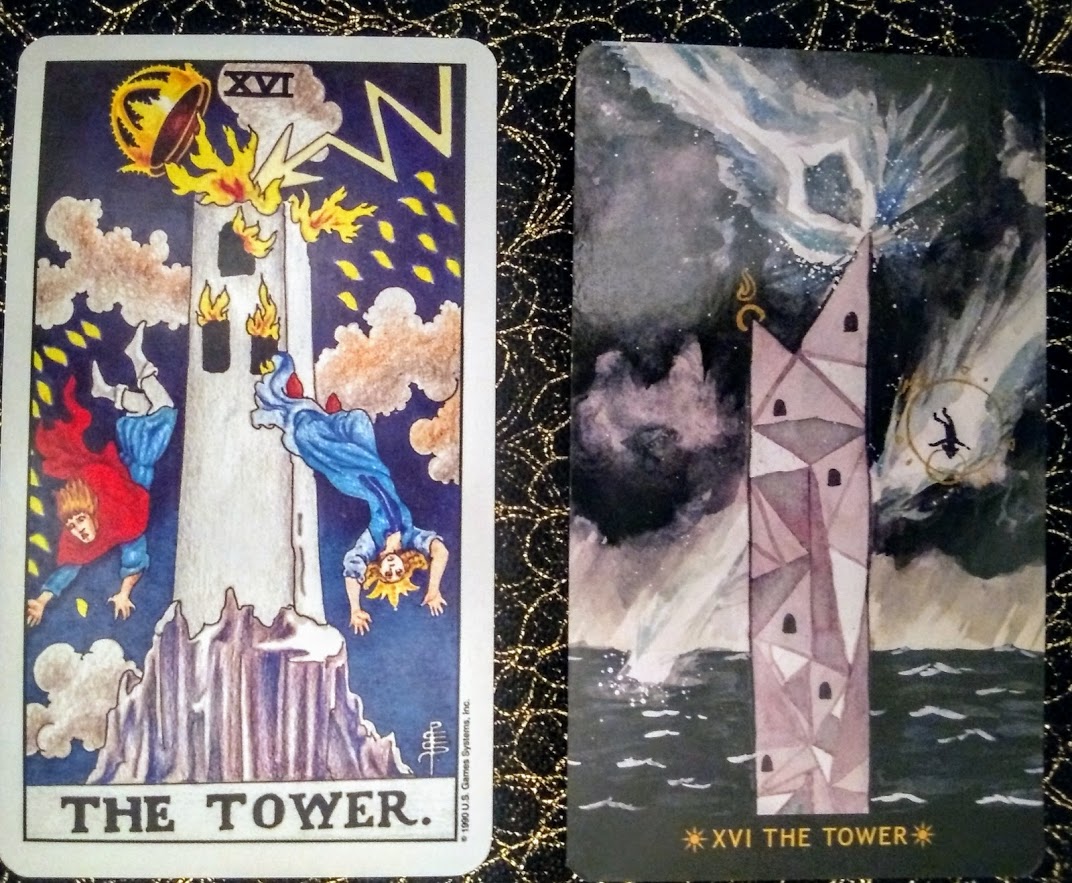 One of the most dramatic (and hence dreaded) cards in the deck, The Tower brings its own deep medicine to our development, being an archetype of both CHANGE and AWAKENING. This card illustrates moments of sudden and unexpected change, violent upheaval, and the collapse of our established structures. We can often feel shattered and shocked by the forces beyond our control that turn our world upside down. This may also appear for us when we’ve cocooned ourselves in denial, refusing to see the changes that need to be made; in this case, it’s our pride, ego, or false sense of security that feels shattered. The Tower and its lightning bolt, however, may also indicate revelatory flashes of insight, as well as the liberation that an epiphany can bring. Our old, rigid belief structures are suddenly dismantled, destructive patterns are torn asunder, and we dismantle what no longer serves us. We no longer have the choice of remaining in our most comfortable illusions about ourselves and the world. And this might be the deepest medicine of The Tower: though our human nervous systems naturally react to and resist such shocks, we can consciously use these events to disrupt what is stagnant, harnessing the cleansing, cathartic energy to push us outside our comfort zone into greater phases of growth. Collapse is scary and painful. Nothing makes that not so. But it can also bring deep clarity, can release us from stuck places, and ultimately set us free onto a new path. The Tower invites us to remember the seeds that only sprout following forest fires, to have courage to face what grows out of chaos, and to be humbled by the workings of the larger universe. (Cards pictured here are from the Universal Waite, a recolored version of the Rider-Waite-Smith deck, and the Numinous Tarot, a radical deck with diverse representations and gender-neutral language.)
My goal in providing this information is not to promote such use, but to assist you in doing so with the least risk and most benefit, should you choose to do so. Please see my Harm Reduction series for more information about reducing risk and habit change.
So: if your party scene involves Special K, what do you need to know to keep everyone safe as possible? (Here's one top tip: try your best not to combine it with alcohol!) Borrowing heavily from Karl Jansen’s excellent book Ketamine: Dreams and Realities (2001), let’s approach specifics for safer use of ketamine through the lens of drug, set, and setting. I'm pleased to share my interview on a podcast about psychedelics and integration!
This local podcaster spoke with an array of community members (including a co-founder of the integration group ERIE, another therapist, media folks, festival attendees), and I think the result is a pretty neat collage-style treatment of the topic. It's likely best listened to in context, but if you're in a hurry, my main segment is at 16:30-24 minutes in (with a few more soundbites at 31:15 - 32:40 and 40:25 - 41:14). Listen here on Google Play What do you think about some of the more controversial topics raised (especially near the finale of the show?) I'd love to hear your feedback, so feel free to share! A log of my continuing education and additional training received. ONGOING: Monthly Somatic Attachment Therapy Practice Group with Karen Rachels, LMFT Monthly Gender-Focused Consultation Group with Lisette Lahana, LCSW June 2019 Queering Psychedelics Conference via Chacruna: moderated a discussion group (2 days of presentations and panels) March 2019 When the Analytic Third Includes a Psychedelic Karen Peoples, PhD, Harvey Schwartz, Phd and Christopher Stauffer, MD January - May 2019 Practice-focused Somatic Attachment Therapy Training, Level One with Karen Rachels, LMFT: 39 contact hours in 6 days November 2017 KRIYA Conference for Ketamine Professionals: presented on panel about setting up a ketamine practice, took notes of all proceedings September 2018 Orenda Institute's Ketamine Assisted Psychotherapy training: 40 contact hours in a 5-day retreat Encountering the Numinous and Need for Integration with Dr. Bryan Wittine August 2018 Bodywork with Medicine workshop Cultural and Political Perspectives on Psychedelic Science at CIIS (2 days of presentations and panels) March 2018 A Really Good Day: A Conversation on Microdosing with Ayelet Waldman February 2018 Introduction to Internal Family Systems with Richard Schwartz November 2017 KRIYA Conference for Ketamine Professionals (2 days of presentations and panels) September 2017 Psychoanalytic Psychotherapy with Gay and Queer Identified Men: Developmental and Cultural Considerations July 2017 Embodied Wisdom: An Introduction to Hakomi Mindful Somatic Psychotherapy April 2017 Well Clinic Refugee Mental Health Consultation and Mentoring Group: Legal and Mental Health trainings MAPS Psychedelic Science Conference (3 days of presentations and panels) -Innovation, Creativity, and the New Psychedelic Culture (workshop) -Integrating Psychedelic Experiences (workshop)
January 2017
Collaborating with Professional Surrogate Partners: A Panel and Workshop Erowid’s Psychoactive Encyclopedia: Earth and Fire of Erowid in Conversation with Matt Tarnas Segall November 2016 MDMA-assisted Therapy for Social Anxiety in Autistic Adults with Alicia Danforth (researcher) and Nick Walker (autism advocate) Notes from a 20-Year Psychedelic Odyssey: Chris Bache in Conversation with Sean Kelly August 2016 Advanced Clinical Work with Transgender Clients May 2016 More Than One Can Live: Reconceiving Harm and Reparation in the Intersubjective World with Jessica Benjamin, Ph.D. Facilitated reading group for CMH clinicians on Benjamin's work to prepare for the training Psychoanalysis in El Barrio: Film and Discussion April 2016 Ethics in Supervisory Relationships via GoodTherapy March 2016 Painting Your Personal Mythology: Expressive Arts Techniques Death, Aging, and the Soul Aroused: Embracing Life's Final Mystery with Charles Garfield at the C.G. Jung Institute December 2015 - February 2016 Variance Institute Series: 4 Workshops about polyamory, kink and clinical issues October 2015 Life Without Walls: The Intrigue and Anguish of Work With Our Homeless Professional Development: Hatching a Private Practice Here's the continuation of my psychedelics discussion. In the first part, we reviewed the resurgence of psychedelic research and how to support those having challenging experiences. As mentioned previously, you may be interested in not just preventing harm, but in getting the most out of your use of these powerful catalysts of consciousness. BENEFIT MAXIMIZATIONThe three critical elements to consider are your intention, how your intention shapes your preparation, and then integration of your experience into your everyday life.
Is your goal relational, such as enhancing intimacy and communication with your partner? If you're wanting to have a really amazing time while at an upcoming festival, your motive may be recreational. Please note that none of these intentions are better than the others (and in fact, we often have a mixture of more than one). Your planning and methods will vary, however, depending on your objective, so awareness is important. Preparation for your journey is key, and is best understood through the lens of drug, set, and setting. (See Part Five in my harm reduction series for a more extensive discussion on this topic.) DRUG: One of the best ways to trip safely is to know what you are taking. If this is a substance that is new to you, please do some research on Erowid (or other sources of quality, unbiased information) so that you are familiar with the typical effects, dosage range, and duration. It may be wise to begin on the low end of the dosage range to see how you react to this new substance. Another important factor is drug purity (for example: how much MDMA is actually in what you're taking?). Pill-testing information (for both MDMA and LSD) can be found at EcstasyData and DanceSafe. Interactions are also extremely important; Zendo volunteers have shared that many of the folks who end up there for assistance have mixed multiple (often unknown) substances together. Again, if you are on any medications, please check in with a health care professional (and do your research) before using psychoactive drugs! SET: Psychedelics are thought of as "non-specific amplifiers," meaning that they can greatly enhance the perception of whatever is already happening for you. Consider your current state: did you just have a difficult breakup and haven't slept for three days? Worried about losing your job? That content will likely come up, so be ready for it. (This may be intentional for those using the medicine therapeutically, but can cause discomfort for those looking to use recreationally.) Awareness of your own personal and family history of mental health is also very important, as those with psychotic or bipolar vulnerabilities may have adverse reactions to these substances. SETTING: Psychedelics are unique in how they sensitize us so exquisitely to our environment, which means that our surroundings crucially shape our journey. Knowing that we will be in a highly suggestible state can help us decide where we want to be and who to have around. Many choose to create rituals to begin and close their journeys, and surround themselves with stimulating artwork or meaningful objects. They plan special music playlists to help guide them through the experience. They trip outdoors in nature, or in private, safe accommodations without risk of interruption. It is also helpful to be deliberate about who else will be involved in your experience. You may choose to be with a intimate partner, or a group of close friends; it can be helpful to make an agreement with everyone beforehand on how to handle difficult experiences. (If there isn't enough trust built to have such a conversation, you might think twice about tripping with these folks!) There are longstanding traditions involving the use of a shaman, trip sitter, guide, therapist, coach, ground control, or otherwise sober person during these journeys. Many feel that they are able to let go and travel to much deeper places when a guide provides a stabilizing, grounding force. Plant medicine use in indigenous cultures tends to be highly ritualized and directed by an elder or shaman, which can help contain the powerful material that can arise. If you are curious about using a sitter, I highly recommend James Fadiman's excellent book The Psychedelic Explorer's Guide, which describes in detail the best practices for guiding/being guided on safe, sacred entheogenic journeys. (Another great collection of resources about trip-sitting can be found here, and you can read the relevant chapters of Fadiman's book in this pdf.) PUTTING IT ALL TOGETHER: let's say your intention is to enhance your enjoyment of a concert with friends. Great! In that case, you might choose a lower dose (i.e. a "museum dose") in order to best facilitate dancing and crowd navigation. You could check in with your friends to see if they will be similarly tripping (or to designate a sober trip-wrangler), and to make a safety plan for the evening. You might also want to be sure that your mental health feels optimal, with no acute stressors, as well as being well-rested and adequately fed before you begin. Make sure you have regular access to water at your event, and pay attention to temperature regulation. Don't operate a motor vehicle. Have fun! However, if your intention is to address longstanding PTSD symptoms and facilitate the healing process, you may choose a much higher dose, and plan both preparatory and follow-up therapy sessions to lay the groundwork for the journey.
Finally, let's now turn to the importance of integration. These medicines can bring profound improvement to our lives when we bring the insights gained during the trip back into our everyday world. A period of introspection following the journey is highly recommended, especially for those with therapeutic and spiritual aims, so giving adequate time for this unfolding is important. There are multiple ways to reflect on your session: journaling about your experience (especially while reviewing your initial intentions), speaking with someone you trust and who understands psychedelic use, creative expression, attending a local integration group, bodywork, meditation, yoga, or spending time in nature. A growing number of therapists are now beginning to offer integration services, and I am happy to be one of them! You may contact me to find out more about how I work, and if I might be a good candidate for your support team. That's all for now! I hope you enjoyed my tiny sample of this immense topic, and please let me know if you have any questions or want to discuss this matter more. Thanks for reading. Disclaimer: These substances remain illegal in many jurisdictions, and this site does not recommend the activities described here. This information is provided for educational purposes only, and to assist those who have already decided to use substances to do it in the safest and most beneficial manner possible. It is your responsibility to assume the risks associated with these activities. Please consult with a medical professional beforehand, especially if you have a preexisting physical or mental/emotional concerns, or are on medication. Psychedelic-assisted therapy is legal only in approved research settings, and I am unable to offer such services at this time.
Welcome back! The next two installments in my harm reduction series concern strategies and techniques best used with psychedelics (such as LSD and mushrooms) and empathogens (such as MDMA). The mainstream media (such as this illuminating New Yorker article by Michael Pollan) has recently given much attention to the resurgence of research on psychedelic- and empathogen-assisted psychotherapy, and the promising results being obtained in treating PTSD, depression, end-of-life anxiety, substance misuse, and other forms of distress. Additionally, a new generation of enthusiasts are buzzing about the magic of microdosing. Many of us in the field are eagerly awaiting our renewed ability (following decades of restrictions) to make use of these powerful change agents, and in the meantime, are attending international conferences and certificate training programs in anticipation of a post-prohibition world.
HARM REDUCTION In response to the needs of our community, organizations such as the Zendo Project aim to create safe, calm environments with trained volunteers to support psychedelic users having difficult experiences, preventing the automatic intervention of law enforcement or medical services.
The Zendo Project has successfully staffed numerous festivals--such as Burning Man and Lightning in a Bottle--since 2012. I've been inspired by their work, and would like to share some of the most important points here. If you happen to encounter someone who is having a difficult trip and are able to assist them, begin by asking about any physical complaints which might necessitate medical attention. You may then find out what they've taken, how much, when they took it, and if they are on any other medications or substances (including alcohol) that might interact. You might then support them using these four principles: 1) Safe Space: These substances often enhance perception, making us extraordinarily sensitive to our environment, and we can easily become overwhelmed by sensory and interpersonal input. If someone is having a challenging experience, you may attempt to move them to a setting that is quiet and comfortable, with enough space for them to feel at ease. Adjust temperatures if they are too hot or cold, and offer water. Soft music and dim lights are helpful. 2) Sitting, Not Guiding: Provide a calm, reassuring, non-directive presence, without feeling the need to "fix" anything. Respond when needed, but don't take over; allow their unfolding experience to guide. Just be with, listen, and observe. Encourage any expression that needs to happen (via conversation, art, dance, movement, sound, etc). 3) Talk Through, Not Down: Help them connect with their feelings, and invite them to gently explore, rather than resist; most difficult experiences are a result of fighting what's happening during the trip. If it is helpful, you may remind them, when needed, that (a) they have taken a drug, and its effects will pass before too long and (b) they are safe where they are, and any medical needs will be attended to. 4) Difficult Is Not the Same As Bad: Where appropriate, you may remind them that many other people have had similar trips, and that challenging experiences often lead to learning and growth. Encourage them to face their experience with curiosity about why these feelings are arising now. (Do you want to see a role-play video of these techniques? Sure, why not?) The intervention of medical or security staff still remains an option in extreme cases, but many are able to resolve their difficult experiences fairly organically and positively when given this type of support. These principles can help someone who is in the middle of a challenging trip, and you might recall them for yourself as needed. (Full credit and gratitude to the Multidisciplinary Association for Psychedelic Studies and to Zendo, a MAPS project, for this important information!) However, perhaps you want both tools to troubleshoot problems, and tips on how to have the most positive experience possible. Benefit maximization is just as important as harm reduction, and I'll cover that in my next post. Go here for the next bite-sized bit on this topic! As we work through our collective open wound of current political heartbreak, I'd like to share with you something small that has sustained me through the years. My old agency held harm reduction-based substance misuse support groups every day. Posted on the bulletin board in our group treatment room was this faded, over-copied sheet of paper*. For nearly a decade, I skeptically stared at these words. I eschewed the idea of a "higher power," and certainly didn't identify with the language of traditional 12-step recovery. I rolled my jaded eyes at its earnest hopefulness, as well as its dated references (faxes? car phones? how very 1991). Eventually, though, I found myself returning to these thoughts for comfort, especially those in #6 and #8: 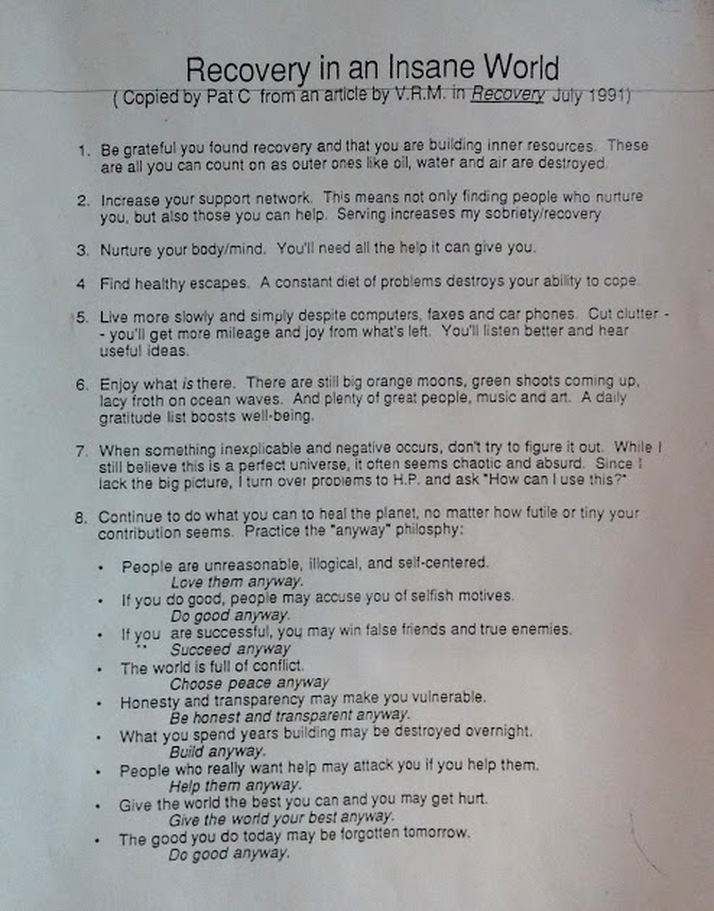 Why did I take a copy of this when I left that agency, and why does it hang on my own bulletin board now?
Because I finally realized that we are all in recovery from something. We are all in a constant state of distress over how living in this world harms us, and we are always working to repair ourselves, and to mobilize hope in each other. I have used these words to inspire my own recovery from: that job, my own bad habits, failed relationships, growing awareness of racism and rape culture, demoralization and hopeless cynicism, national tragedies, and so much more. Now, in this time of toxic stress and fear for our future, let Laurie Penny remind us that self-care and mutual support can be tools of resistance...and that though we may face seemingly insurmountable odds, we are still called to do it anyway. Be well. * I regret that I have been unable to discovery the true origin of these words--Pat C? V.R.M.?--so if you happen to have an idea about how to correctly source this piece, please let me know! |
Jessica Katzman, Psy.D.I'm a psychologist with a private practice in San Francisco's Castro District. I'm interested in harm reduction, LGBTQQIAAP issues, psychedelic integration, social justice conversations, size acceptance, and any intersections of the above. I welcome your comments! 
Photo credit: Tristan Crane Photography.
Categories
All
Archives
June 2020
Disclaimer: The information and resources contained on this website are for informational purposes only and are not intended to assess, diagnose, or treat any medical and/or mental health disease or condition. The use of this website does not imply nor establish any type of therapist-client relationship. Furthermore, the information obtained from this site should not be considered a substitute for a thorough medical and/or mental health evaluation by an appropriately credentialed and licensed professional. This website includes links to other websites for informational and reference purposes only. This website does not endorse, warrant or guarantee the products, services or information described or offered at these other websites. Examine the content carefully.
|





 RSS Feed
RSS Feed